

How can government drive more medication development for addiction? Our work in DC.
CASPR gets FDA acceleration language for SUD into the House Appropriations Committee report.

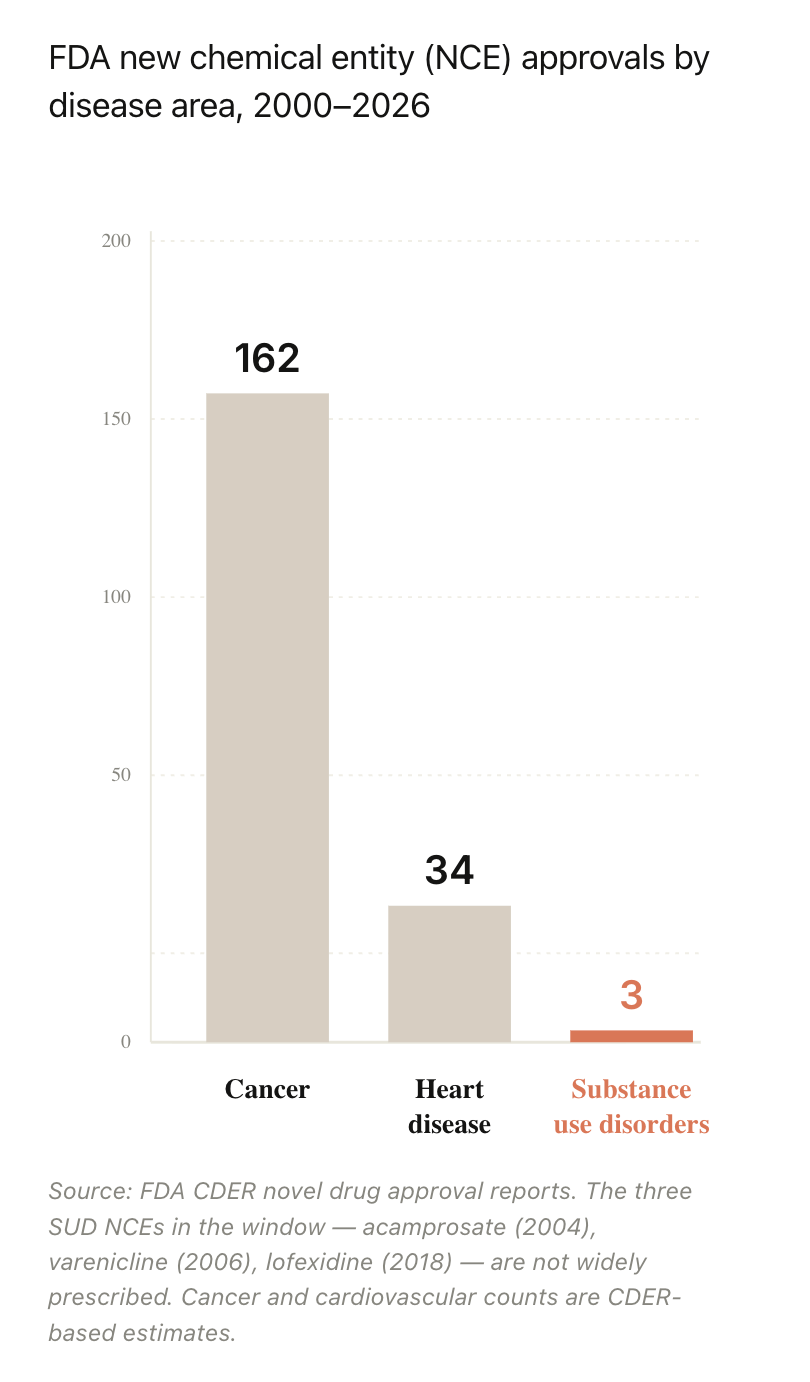
Why are there so few approved medications for addiction? 48.4 million Americans have a substance use disorder, making it one of the most common disease areas in medicine. And 37.8M smoke cigarettes. These addictions drive more deaths and disease than either cancer or heart disease (including by causing a significant portion of cancer and heart disease). Shouldn’t addiction be a hugely successful area for pharma companies?
Yes! It should! But instead, addiction medication development has been a desert. While new buprenorphine and narcan formulations have played a very important role in opioid treatment over the past 20 years, there have been no widely adopted new molecules in the field in decades:
CASPR’s core thesis, which drives our mission, is that we cannot permanently solve addiction at scale without new breakthrough medications. The treatments we have currently in each addiction indication are either not sufficiently effective or are very unappealing to patients, even in places where access is high.
Ten years ago, obesity had the same problem. There were approved FDA treatments for obesity but they sucked. They had too many side effects, the efficacy was too low, and patients didn’t stay on them. Pharma invested very little, until… semaglutide arrived for diabetes and went viral among patients for its weight loss effects. Now there is a massive pipeline of next-generation obesity treatments coming to patients. And it’s changing society. For the first time, obesity is falling every year in America.
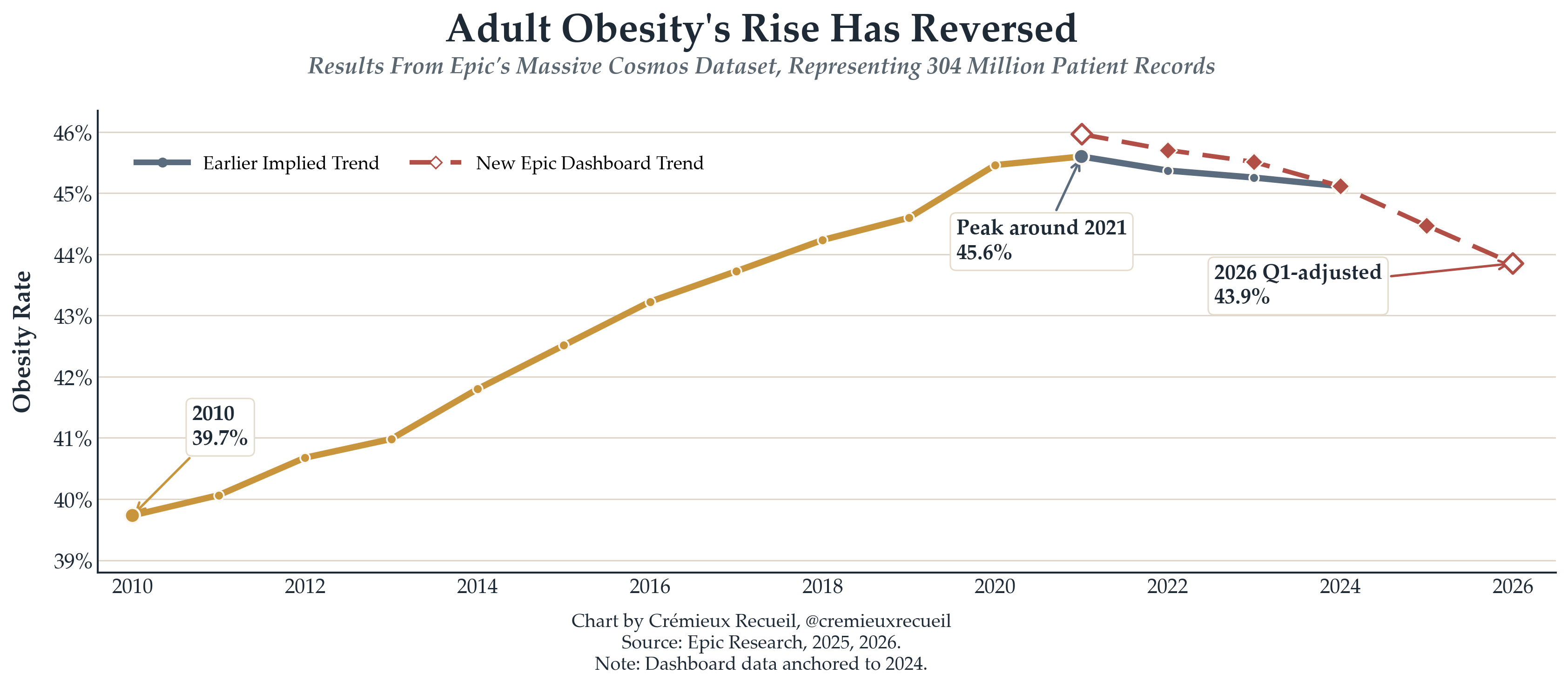
As GLP-1s for obesity become generic and access increases, this trend will accelerate. It is one of the most important public health achievements in history.
Can we make this happen in addiction?
As we’ve been building CASPR, we’ve talked to hundreds of research scientists, biotech investors, biotech founders, and pharma executives about why there is so little medication development.
Since addiction is so widespread and so devastating to individuals and families, this should be a huge opportunity for pharma companies. So why aren’t we being bombarded with ads on TV for new and better anti-addiction medications?
The biggest obstacles are:
Existing SUD medications are not perceived as financially successful. Pharma is extremely risk averse compared to other industries (which often causes companies to miss opportunities like they did in obesity). For biotech investors, a disease area with very little competition looks like a warning sign, not a wide open opportunity.
Running trials on people with substance use disorders is risky. What if an OUD patient dies during a trial and it gets blamed on your treatment? Pfizer was sued for an anti-smoking treatment, Chantix, that people believed increased suicide risk, paid out $273M in settlements, and studies later showed no increased suicide risk.
FDA endpoints for addiction trials have focused on patients achieving abstinence. This creates something of an all-or-nothing bar for new treatments to cross. In other disease areas, like cancer, very modest improvements in remission and survival, on the order of months, are approved by the FDA because it’s expected that medications will be layered together. Addiction needs the same orientation towards treatment. Today, when biotech investors consider an investment in an addiction, they quickly run into concerns about whether the drug will be approved by the FDA if the efficacy is modest but not amazing. This increases the risk that the investment will fail and leads them towards other disease areas.
All of the above have created a reinforcing cycle of neglect. Because investors have not funded addiction medications in the past, they don’t understand the market and don’t have confidence evaluating it. Because pharma companies don’t have existing addiction medicine programs, they lack the staff to assess new opportunities and are much less likely to acquire new companies in this space. If pharma won’t acquire, investors become even more averse to investment. New companies simply can’t get off the ground.
This problem is the core focus of CASPR’s policy work and lobbying, the foundation of our Innovation Agenda for Addiction. We believe better medication is path to get from 3% of people with a substance use disorder receiving medication to 10%, 20%, 30%, and beyond. Better medication is how we will permanently reduce the incidence of addiction around the world. Breakthrough medications are how we will find cures, at the level of both the individual and society. But we have to get that flywheel spinning.
Key levers from our Agenda:
Modernization of FDA endpoints for substance use disorder approvals.
Accelerated FDA pathways for new addiction medications, which reduce cost and time to market.
Creation of a Priority Review Voucher program for addiction indications, which has spurred medication development in other under-invested disease areas.
Our Progress in Congress
Last year, spearheaded by Caroline DeBerry, who leads our efforts in DC, CASPR succeeded in getting language into the Senate L-HHS FY2026 appropriations committee report pushing the FDA to improve endpoints:
Although there are effective medications for treating opioid, tobacco, and alcohol use disorders, these treatments do not work for everyone — and to date, no medications have been approved by FDA to treat stimulant use disorders. The Committee therefore encourages FDA and NIDA to collaborate on the establishment of endpoints other than abstinence for use in clinical trials of medications to treat substance use disorders. Such alternative endpoints may include reduced craving (defined as a strong desire or urge to use drugs), reduced drug use, or reduced substance use disorder severity. The Committee appreciates NIDA-funded research on using alternative endpoints in clinical research on substance use disorders, such as the recent finding that reduced drug use is associated with meaningful clinical improvements for people with stimulant use disorders. The Committee urges FDA and NIDA to build upon such research and work together toward incorporating alternative endpoints into clinical trials for substance use disorders."
This week we made more progress, placing language in the House Appropriations Committee report that accompanies the FY2027 Agriculture/FDA appropriations bill. In case your memory of page 81 of this report is a little fuzzy, here it is:
Accelerated FDA Reviews for Substance Use Disorder Treatments.—The Committee encourages FDA to explore and, where appropriate, implement accelerated review approaches for qualifying substance use disorder treatments, including priority review, fast track designation, breakthrough therapy designation, and other expedited programs authorized under current law and available to the Commissioner. The Committee further encourages FDA to evaluate whether additional regulatory tools or administrative pathways could reduce development and review timelines for high impact addiction treatments while maintaining rigorous standards for safety and efficacy.
(Emphases mine to help spare the reader.)
While these statements are not legislation and do not require specific actions, they do communicate the goals and intent of Congress and are highly influential at these agencies. We are also pursuing legislation, as we keep pushing on every lever we can to advance innovation in addiction medicine. Please take a look at CASPR’s policy priorities.
And one final note that’s worth repeating: CASPR is a true grassroots non-profit, we do not take money from pharma or biotech, we are funded by foundations and families affected by addiction. We deeply believe that after decades of political tug-of-war over the drug war and endlessly agonizing policy debates about drugs and society, the path to truly solving addiction requires breakthroughs in medication development.