

Making a non-opioid painkiller available to everyone would save Medicare and Medicaid $14.9B and prevent hundreds of thousands of new addictions
Suzetrigine is sitting on the shelf waiting for its patent to expire, while hundreds of thousands of new opioid addictions are being caused by unnecessary opioid prescriptions

The role that Purdue pharma and the Sacklers played in the opioid crisis, lying to and manipulating both doctors and regulatory agencies, has been well-documented. These were profound failures of both industry and government. But at the core of what went wrong, and what enabled such profound mistakes at such a large scale, was a sincere desire among doctors (most of them, at least) to relieve the torment of pain for their patients. It’s easy to say oxycontin was overprescribed and demand that things change, but it’s a lot harder to tell someone that you won’t treat their pain. And the price of pain should never be glossed over— nothing destroys happiness and freedom as quickly as pain does. Every day doctors still face the impossible dilemma of whether to provide pain relief while putting their patient at risk for addiction.
But now for the good news!
Suzetrigine is a non-opioid, and truly non-addictive, painkiller approved by the FDA last year, a drug that can potentially replace 51% of opioid prescriptions and prevent a huge portion of new opioid addictions. It’s not the strongest pain medicine, but its comparable to hydrocodone (aka Vicodin), which is widely used for mild or moderate acute (aka short-term) pain treatment. The problem is that suzetrigine is a new, on-patent drug with a high price, and very few patients can get coverage today.
This spring, CASPR published a policy paper on suzetrigine access arguing that the federal government should negotiate a lower price for suzetrigine in exchange for making it a first-line treatment, available to everyone as easily as hydrocodone is today. In fact, it should become easier to get suzetrigine because it’s not a controlled substance.
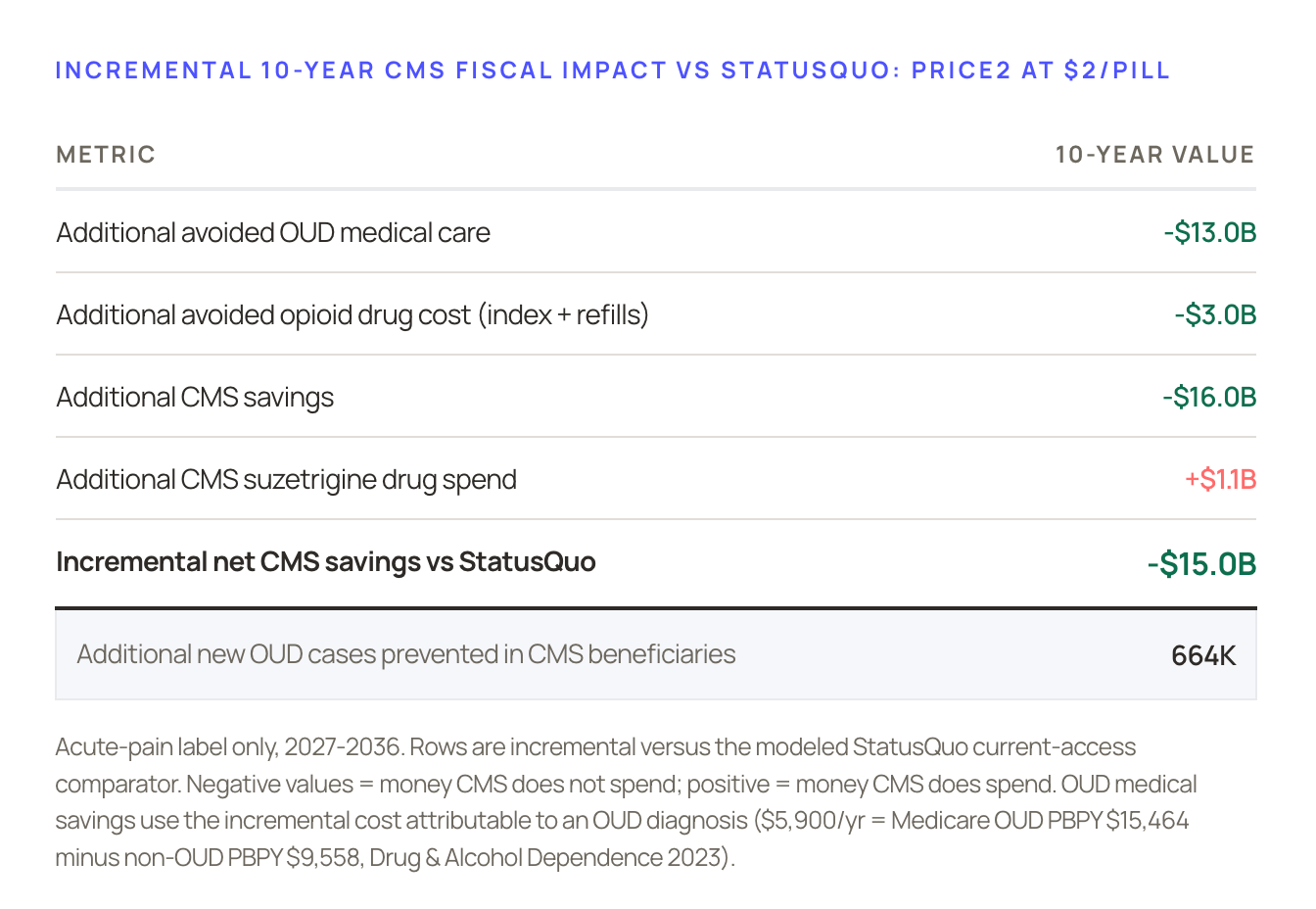
Today we are publishing a detailed fiscal analysis and impact projection that we built based on this proposal:
10-Year CMS Cost Impact of Negotiated First-Line Suzetrigine Access
If you aren’t a policy wonk, that might not sound like a very exciting headline, but you might find the charts a lot more compelling than you’d expect.
Trading price for access
Suzetrigine is cheap to manufacture which means that the drug company, Vertex, can make an equivalent profit at a much lower per-pill price if they can reach far more patients. By reducing the price from $15/pill to $2/pill, Vertex would do well and the government would save $15B over ten years in CMS (which is Medicare and Medicaid). The cost savings come primarily from preventing opioid addictions, which are extremely expensive to treat.
The savings increase by >10X if you include downstream social savings from avoiding early death, unemployment, disability, crime, incarceration, and more. Most importantly, we can prevent hundreds of thousands of new opioid addictions:

We believe our proposal is a rare win / win / win for the government, the public, and Vertex, and can serve as a model when other companies bring more non-addictive painkillers to market. There’s no good reason that we should be waiting 14 years for suzetrigine’s patent to expire before we stop creating so many new opioid addictions.
Here’s the link again to the fiscal analysis: Cost Impact of First-Line Suzetrigine Access
And, as always, it’s important to say that CASPR is a true grassroots non-profit organization, not funded by pharma or biotech. We believe advancing breakthrough medicines for addiction and pain is the key to solving addiction at scale.
And one more chart:
