

Addiction predictions: How did I do for 2025?
I did... ok? decent? pretty good?

Last year I made a series of Addiction Predictions for 2025 and beyond. Let’s see how things went:
Suzetrigine, a novel non-opiod painkiller, will be FDA approved for acute pain in January 2025: 90% chance.
CORRECT: Suzetrigine was approved on January 30. Use of suzetrigine has been very limited because it is an expensive on-patent drug. This mean millions of unnecessary opioid prescriptions are continuing to be given to patients. I’ve written in the past that the federal government should make a deal with Vertex to reduce the price in exchange for vastly increased access, making suzetrigine a first-line pain treatment (and replacing most uses of Vicodin). This would rapidly reduce the number of new opioid prescriptions written every month, by up to 50%. We’ll be publishing a more detailed proposal about this soon.
Suzetrigine will be seen as a modest step forward for pain management but will spark excitement and vision towards a future of opioid-free outpatient pain management: 70% chance*.
CORRECT: The asterisk on this and other predictions means that the outcome is fuzzy and doesn’t have a clear objective answer. But I think this one is true— suzetrigine is an important step for the field and for opioid replacement, but we’ve heard that many prescribers just don’t think it’s strong enough to be worth the hassle of prescribing it vs ibuprofen / acetaminophen.
Two or more Phase 2 RCTs will report results showing a large drop in heavy drinking among people with AUD who take semaglutide or tirzepatide: 90% chance.
HALF WRONG: Christian Hendershot’s highly cited trial of low-dose semaglutide for AUD showed a big drop in heavy drinking but it was the only AUD sema / tirzep RCT released last year (that I know of). That said, there are a handful of AUD sema or trizep trials that have completed but not yet published results, so there should be more papers this year.
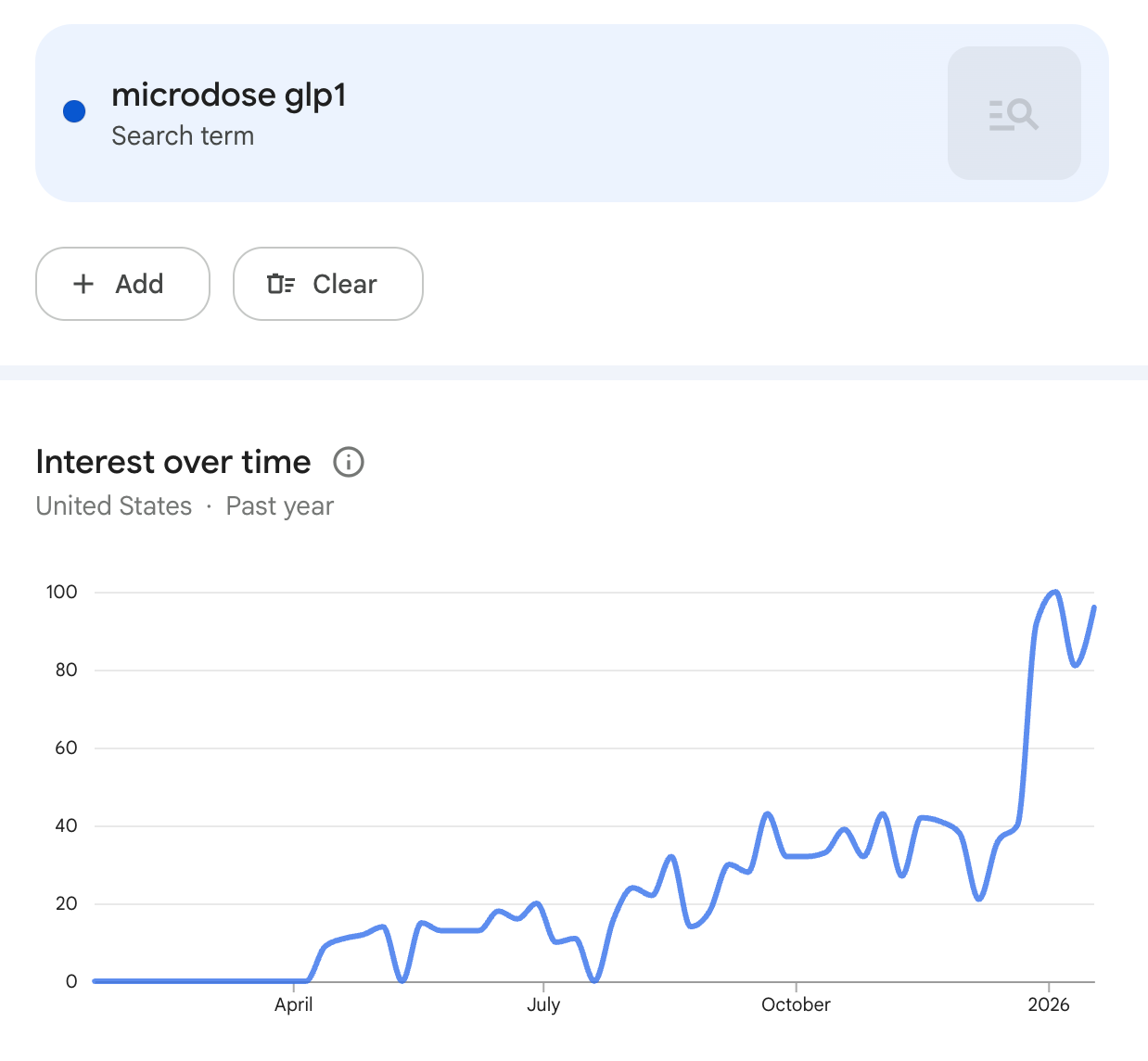
“Micro-dosing” GLP-1s (for weight, addiction, hormonal regulation, brain health, etc) will grow from a small niche to a large trend: 70% chance*. Micro-dosing will serve as the psychological bridge that lets alternative medicine advocates embrace GLP-1s. The trend could stall within the US if compounding of semaglutide is shut down.
MESSY: Microdosing GLP-1s is certainly growing in popularity (see the google trends chart below) but I think objectively it remains below the level of a ‘large trend’. That said, I think it will continue to grow and there has been a lot of coverage of the concept recently (here’s the Today Show).
Semaglutide compounding will be shutdown: 50% chance. The law and Novo’s business interests point to a shutdown, but Makary (upcoming FDA head) was CMO of a compounding service and the many millions of people who are currently taking compounded semaglutide will be driven to unregulated gray market alternatives from China if compounding is stopped.
MESSY: Most GLP-1 compounding shut down in 2025 but several services remain alive and well. Novo and Lilly continue to sue companies and try to stamp it out but there are ongoing court battles from compounders who argue that they are providing custom medications that people can’t get elsewhere. Compounding has played a big role in the price reductions for patients paying out of pocket.
At least one telehealth service will begin offering compounded semaglutide off-label for substance use disorders: 60% chance. (I would have a higher likelihood if it wasn’t for the risk of compounding being shut down at some point in 2025.)
MESSY: WorkIt Health temporarily launched a GLP-1 for addiction service but it is no longer active. That said, if I was making predictions again, I’d re-predict this for 2026. It’s coming one way or another.
Incretins as the future of addiction medicine will go from what was a niche belief at the beginning of 2024 to the mainstream position of addiction experts by the end of 2025: 70% chance*. But it will continue to take a long time for research in the field to pivot proportionally to the opportunity.
CORRECT: GLP-1s for addiction have had far more attention and adoption this year than any other novel addiction medicine and NIDA is increasing its funding of GLP-1 trials, though still far too slowly in my opinion. Eli Lilly has launched a GLP-1 for AUD phase 3 program with brenipatide, which is a major step towards mainstream access. CASPR is also working to launch a phase 3 program, I hope we’ll have more news here soon.
Overdose deaths will continue to drop in 2025 vs 2024, by at least 5%: 75% chance.
CORRECT: Overdose deaths had another huge drop in 2025, down by 20.6%. Wonderful.
Why did deaths keep dropping? We still don’t know. I wrote last year about the possibility that the drop was driven by a trend away from injecting fentanyl towards smoking fentanyl, others have proposed that the gradual increase in availability of naloxone and buprenorphine has been making an impact, and others suggest the huge overdose surge during covid is just leveling off. An excellent paper in Science last week suggests that a ‘China shock’ of new restrictions on fentanyl precursors caused a drop in the strength of street fentanyl that corresponded closely with the drop in overdose deaths.
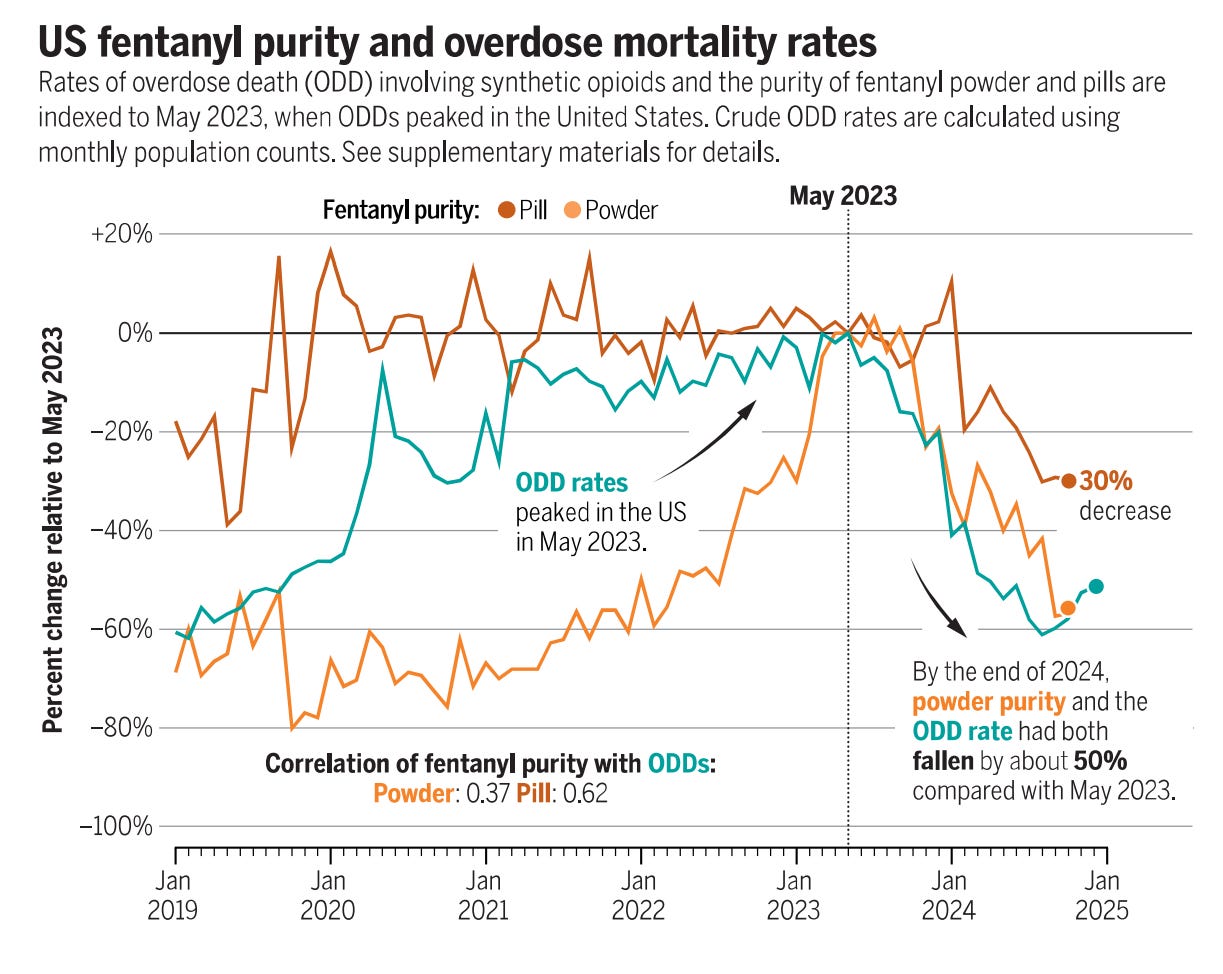
This correlation seems pretty convincing to me, though the other theories remain plausible and contributory to various degrees.
Like me, the vast majority of addiction medicine experts and professionals are not in favor of the drug war and are skeptical that the opioid crisis can be solved on the supply side. I think supply shocks like this will be hard to maintain and other countries will fill in the precursor gaps if China continues a crackdown. It’s just too easy to make fentanyl. But despite this justified skepticism of supply-side restrictions it’s important to remain open-minded to the role that supply plays and to be open about our uncertainty. It is certainly possible that the right international coordination could choke fentanyl supply significantly, leading to a big rise in prices and a drop in purity and a reduction in deaths. Again, I think it’s unlikely, but we should “follow the science” on this and everything.
The overdose death drop from 2024 to 2025 will be lower in percent terms than the drop from 2023 to 2024: 70% chance.
CORRECT: The 2023 to 2024 drop was 26.9%, and this year’s drop was 20.6%.
Someone you know personally will tell you that they drink a lot less since starting a GLP-1: 96% chance.
CORRECT? You’ll have to answer this one yourself. It happened to me about 6-7 times in 2025 but I am constantly having these conversations.
Novo Nordisk’s EVOKE trials of semaglutide for Alzheimer’s report positive results in late 2025 or 2026. They will show reduced Alzheimer’s incidence in people taking semaglutide, including individuals without diabetes or obesity: 80% chance.
WRONG: “While treatment with semaglutide resulted in improvement of Alzheimer’s disease-related biomarkers in both trials, this did not translate into a delay of disease progression.” - Novo Nordisk press release. I hope Novo will release more details of their results, including subgroups, but overall the trials clearly failed. Long-term I still suspect that for people with diabetes or obesity, we will see strong evidence that GLP-1s reduce Alzheimer’s incidence. But it’s virtually impossible to run a 10 or 20 year RCT prevention trial (this is a problem for all Alzheimer’s research).
Success of EVOKE will eliminate most of the remaining resistance towards GLP-1s as a ‘crutch’ or ‘bandaid’ for people with diabetes or obesity: 70% chance*.
WRONG: The trials failed! That said, I think that GLP-1 skepticism and resistance is continuing to drop rapidly as the popularity grows, people see their friends having success, and more data shows broad health benefits and reduced mortality.
So how did I do?
I think I did… decent? On the bigger trends I was mostly right, with some details and timings off, and too much hopefulness on Alzheimer’s, where I have a lot of family history.
I still have a few more predictions pending for 2027 and beyond.
The past few months I’ve been overloaded with new policy and research projects that CASPR is preparing to launch and my head has not been in mindset to make new predictions. That said, 2026 will certainly be a big year for GLP-1s in addiction medicine as more trials announce results and industry activity grows, getting us closer to an eventual FDA approval.
Really solid self-assessment here. The connection between fentanyl precursor restrictions and overdose death drops is interesting but like you said, probably not a long-term solution. I actually saw a friend cut way back on drinking after starting a GLP1, so that prediction definitely rang true for me. The failed Alzheimer trials are dissapointing though the biomarker improvements without clinical effects suggest timing might be key.