

An Innovation Agenda for Addiction
from CASPR and Institute for Progress (IFP)


Published by CASPR (that’s us) and Institute for Progress (IFP). See IFP’s page for the agenda and the list of authors and collaborators. Also published in a shorter form by the Federation of American Scientists, here.
Policy efforts to address addiction have stalled
Over the past two decades, addiction policy efforts on both the left and right have struggled to reduce harms from opioids, alcohol, and stimulants. For opioids, cocaine, and methamphetamine, the problem has grown many times worse, with overdose deaths near record highs, particularly as these drugs have become widely used in combination. Deaths from alcohol per capita have doubled since 1999 and continue moving upward. No American city or state, no matter how liberal or conservative, has found a solution that can reduce the rate of addiction at scale.
On the enforcement side, it is virtually impossible to stop fentanyl or methamphetamine smuggling. No one is considering an alcohol ban, and attempts to raise alcohol taxes have failed in both red and blue states. While treatment efforts help many people and “medication-first” is considered the standard of care, the medical options currently offered are unlikely to ever reach scale. Only 3% of people with a substance use disorder take medication in a given year, due to existing medications’ limited appeal, efficacy, and availability. For several substance use disorders (methamphetamine, cocaine, and cannabis), there are no FDA-approved medications at all.
US policymakers need a new approach to addiction policy, oriented towards advancing innovation in medication development.
Asymmetrical innovation in addiction
Rapid innovation is happening in the field of addiction, but it’s been occurring on the wrong side: addiction-inducing technologies are becoming more powerful.
Fentanyl is cheaper than heroin, 25x stronger by weight, and therefore 25x smaller for smuggling purposes. Fentanyl is also more addictive, and fentanyl overdoses are more difficult to reverse. As fentanyl has come to dominate the opioid supply over the past 10 years, overdose rates have risen dramatically. And even newer synthetic opioids are also becoming common. At the same time, advances in methamphetamine production techniques in Mexico led to increases in quantity and purity, increasing the strength per gram. Compounding the problem, fentanyl is easily combined with meth and cocaine in pills and powder.
Together, these three innovations (fentanyl, cheap meth, and new combinations) drove a 400% increase in overdose deaths over the past 20 years (see Appendix for more). Without equally powerful innovations to reduce addiction rates, the US is unlikely to make long-term sustainable progress on this problem. Unfortunately, there is very little industry activity in addiction medicine at present, due to modest sales of existing addiction medicines and perceived reputational risks that have created a reinforcing cycle of canceled programs and minuscule venture investment.
Our proposals would incentivize innovation in breakthrough treatments through regulatory incentives, modernizing approval standards, and increasing public funding for addiction medicine R&D. These policies have the potential to permanently reduce addiction at a population scale. Specifically, we propose:
Extending existing incentives for underinvested disease areas to include substance use disorder indications
Rewarding successful approvals in the field
Modernizing and clarifying FDA efficacy standards
Increasing public funding for addiction medication development
Advanced commitments or risk sharing for candidate medicines
Adopting a strategy-first funding approach
Developing public-private partnerships that enable medication development activity
None of the frameworks that have defined policy debates around addiction in recent decades have succeeded in reducing addiction or overdose deaths. Alcohol taxes, the “drug war,” incarceration, harm reduction, decriminalization, and opioid replacement medications are controversial and politically-charged topics, and risk distracting us from the fundamental necessity of new treatments. The recent null results from a large study of a suite of overdose interventions is a warning that the tools available today are not nearly enough, even when implemented effectively — we need breakthroughs.
Between the polarized camps on addiction policy is an achievable, non-partisan path: better medicines.
Reducing rates of addiction has tremendous economic and social benefits, but most of those benefits occur outside of the medical system, which means the value generated can’t be captured by pharmaceutical or insurance companies. This leads to overall levels of investment in new treatments far below their expected social value. By redesigning the incentives of the dysfunctional addiction medicine market, we can put ourselves on a path to permanently solve addiction for individuals, families, communities, and our country as a whole.
Addiction is the most significant medical challenge of our society
The scope of the problem is vast: roughly 750,000 Americans die every year from tobacco, alcohol, opioids, and stimulants. Compare this to heart disease at 695,000 deaths and cancer at 609,000 deaths (and consider that alcohol and cigarettes cause many cancer and heart disease cases). But the cost of addiction goes far beyond the burden of death, disability, and disease for patients themselves. The Council of Economic Advisers estimates that the opioid crisis alone costs the United States $1.5 trillion annually in direct spending and lost productivity.
Even those large estimates likely underestimate addiction’s costs. Addiction tears apart relationships, marriages, and families and drives discord and distrust in communities. More than 321,000 children have lost a parent to a drug overdose in the past 10 years. Many more suffer from their parent’s chronic alcohol and substance use. Roughly 60% of all crimes and 65% of violent crimes are related to drugs or alcohol in some way. Addiction has triggered mass incarceration and a drug war with many unintended consequences. While society is making progress on reducing cigarette smoking through taxes, regulations, and alternate sources of nicotine, there are still 28 million smokers in the US. Smoking still kills hundreds of thousands of Americans per year, and the 1-year efficacy for medications like Chantix (for smoking cessation) is less than 20%. Meanwhile, trends for other substance use disorders have worsened substantially.
The goal of reducing harms from addiction should be a top priority of the nation’s medical system. Yet it is profoundly neglected.
The addiction medication market is broken

Despite the enormous medical, economic, and societal cost of addiction, the field of addiction medicine has been largely abandoned by the pharmaceutical industry and underfunded by the US government.
Between 2000 and 2023, the FDA approved 222 distinct products for cancer, 57 for heart disease, and dozens for psychiatric illnesses. But it approved just 6 for substance use disorders. Of those 6, 3 were different delivery methods for buprenorphine.

The last significant FDA approval for opioid use disorder (OUD) was Suboxone in 2002. Methadone, the other leading medication for OUD, came into use in the 1970s for opioid addiction and has been mired in controversy and regulations ever since. Patients are wary of both medications due to side effects like tooth decay and disrupted sleep, and are often reluctant to use a medication that is itself opioid-based.
Meanwhile, opponents of opioid-based addiction medicine impose highly restrictive regulations that limit access to these lifesaving treatments. The result is that most OUD patients refuse to accept medication, do not remain on the medications long-term, and have very high relapse rates after discontinuation. In a recent six-month trial comparing extended-release naltrexone to buprenorphine-naloxone, more than half of patients in both groups suffered a relapse — thus, even with higher initial uptake of currently approved medications, opiate use would still remain an important problem. Even as some restrictions have been lifted, prescribing rates have remained low.
For alcohol use disorder (AUD), the last major approval was acamprosate in 2004. Acamprosate requires dosing three times a day and has very modest efficacy. It is not widely used. The most commonly used medication for AUD is naltrexone, which also has limited effectiveness, reducing heavy drinking days by only about 5%-18%. This lack of appealing treatment options is disappointing for a disease that harms tens of millions of Americans every year, but is also unsurprising given the low levels of investment in new product development.
A Biotechnology Innovation Organization (BIO) report on pain and addiction medication development was unable to even calculate a success rate for addiction medication approvals because there have been so few in recent years:
“Novel addiction treatments have the lowest Phase II success rate, with 14 of 15 Phase II programs failing over the last decade. The lack of recent Phase III transitions made it infeasible to calculate an overall success rate for addiction.”
The only treatment in its list that has succeeded in achieving an FDA approval in recent years, lofexidine, is rarely used and does not treat addiction itself but reduces withdrawal symptoms. This FDA approval has had no meaningful impact on addiction treatment because generic clonidine has the same effect, is 98% cheaper, and has already been in use for decades for the same purpose.
The comparison to cancer medication development funding is stark. “Venture investment into companies with novel addiction drug programs over the last 10 years is estimated at $130M, 270 times less than oncology,” the BIO report finds.
That means addiction medication receives 0.4% of the venture investment that cancer does, even though addiction in aggregate causes more deaths. This may partially explain why there are consistent, life-extending breakthroughs being approved in oncology but not for substance use disorder. Though cigarette and alcohol addictions are responsible for about 34% of cancer deaths and 85% of lung cancer, pharmaceutical companies spend far more developing medications for lung cancer than medications to stop smoking.
Moving upstream to stop smoking would have a larger impact on individual and public health, and would generate cost savings in treatments avoided downstream. Pharmaceutical companies may correctly believe that they can earn more from new lung cancer medicines than anti-smoking medicines, but the financial and human value to the public of preventing a case of lung cancer is enormous. It is rational to highly incentivize, and even subsidize, development of medications for prevention.
The private sector is not alone in prioritizing downstream intervention. The federal government spends roughly $50 billion every year on drug enforcement, treatment, and incarceration. By contrast, it spends less than $700 million on addiction medication development research (and arguably much less, depending on which National Institute of Drug Abuse (NIDA) and National Institute on Alcohol Abuse and Alcoholism (NIAAA) projects one considers “medication development”-related). Because of industry’s lack of interest in SUD, the field sees a higher-than-average reliance on academic trials, many funded by NIDA and NIAAA, compared to the higher rates of industry sponsorship observed in other research domains.
Public funding is limited and takes too long to access. In a recent conversation, a researcher working on one of the most promising new opportunities in addiction medicine told us they must wait 12 months to receive a roughly ~$140,000 planning grant for a modestly-sized study. That study will then need separate grants to be run. Though not a problem unique to addiction medicine, it is especially important in a field reliant on public grants.
Addiction is a hard science problem, but we spend far less on addiction medicine development as a society compared with other complex and challenging diseases like heart disease and cancer. Predictably, we get far fewer results. Without robust private-sector activity and federal funding for addiction medicine development, we are unlikely to make long-term progress.
Better medication for addiction will save money at all levels of government. Given the social, economic, and border impacts of the war on drugs and addiction, we should invest more in addiction therapy development to reduce the harms of addiction, and perhaps prevent substance use disorders, thereby reducing the need for the tens of billions of dollars in annual funding spent on drug enforcement, law enforcement, incarceration, medical costs, and rehabilitation services.
Why pharmaceutical companies avoid addiction medication development
Large pharmaceutical companies avoid substance use disorder medication development almost completely. They anchor on the low sales of currently available treatments and are wary of the historically low rate of successful approvals for addiction medications. Interested companies must also grapple with outdated and unpredictable efficacy standards set by the FDA for substance use disorder indications. These standards pose a high risk of failure to achieve approval, even for treatments that show clinically meaningful reductions in substance use.
Developing addiction medication can be challenging scientifically due to the range and complexity of potential neurological targets, the variety of addictive substances, and the safety and ethical complications of studies. Clinical trials of addiction medicines are expensive and can fail for a wide range of reasons. For example, recruiting people to participate in an opioid use disorder trial is difficult — researchers need patients stable enough to complete a trial, but draw from a population with high levels of instability. While these obstacles are real, many other disease areas are just as difficult to study for other reasons, and often more so. Trials for challenging diseases like cancer, HIV/AIDS, and diabetes have succeeded through sustained investment from the public and private sector.
Beyond the logistical challenges, large pharmaceutical companies worry that having an addiction program will taint their overall brand or specific products with the stigma of addiction, or will invite criticism that they are profiting from a crisis that the pharmaceutical industry is seen to be broadly culpable for.
These points were a consistent refrain during our interviews with senior pharmaceutical executives and are longstanding. The same issues around medication repurposing that are discussed in this National Academies book still apply today:
“The societal stigma of developing and marketing a medication for treating drug-dependent patients is a concern for pharmaceutical companies. They fear that, once a medication is approved for use in the treatment of drug addiction, the market for other indications will diminish or disappear. Eli Lilly's experience with methadone illustrates the point. Methadone was developed as an analgesic, but its use for pain relief significantly diminished once it became widely used as a treatment for heroin addiction. Patients, in general, do not want to take a medication associated with drug addiction. Thus, the pharmaceutical industry is understandably reluctant to develop compounds specifically for drug addiction, if other medical uses for the compounds are possible.”
While not unique to substance use disorder medications, there have been serious and sometimes unwarranted criticisms and lawsuits directed at the developers of novel addiction medications. In 2013, Pfizer paid $273 million to settle lawsuits related to reports of adverse psychiatric events from Chantix. Following these reports, the FDA added a black box warning to the medication. Pfizer, however, ran an additional RCT that found no effect on psychiatric events. As a result, the FDA removed the black box warning, but the settlements had already been paid. Since Chantix, Pfizer has not pursued development for any substance use disorder medications.
Pharmaceutical companies are also concerned about the complexity of working with patients who are at high risk of suicide and erratic behavior. Companies worry that a drug trial could have patients who die while enrolled — not because of candidate drug toxicity, but because the baseline rate of overdose death and suicide is high in these populations. While these fears have some justification, scientific leaders in the field are frustrated with pharmaceutical companies’ avoidance of this work. As Keith Humphreys, Professor of Psychiatry at Stanford University, told us, "The world's largest pharmaceutical companies have completely divested from developing treatments for addiction other than to tobacco. They have overstated fears of stigma damaging their brand and of liability problems. As a result, the speed of pharmacotherapy progress in the past 20 years is a bare fraction of what we see in other diseases."
Even the seemingly low-hanging fruit of drug repurposing is not risk-free for drug companies. Companies considering label expansion for drugs like Ozempic or Mounjaro, which have promising early in-human data, face an obstacle known as the “problem of new uses”: clinical trials of an already lucrative drug for a new indication carry downside risk if new side effects or adverse events are reported.
The combination of private and public sector neglect has left us, unsurprisingly, with very limited and unappealing medications to offer addiction patients. Overall, the result is that only 3% of people with substance abuse disorders take the medications that are currently available.

If the pharmaceutical industry avoids work in the field of addiction because it responds rationally to incentives, then the value to the public of policy changes that spur pharmaceutical companies to enter the field could be massive.
The medical potential for reducing addiction is high
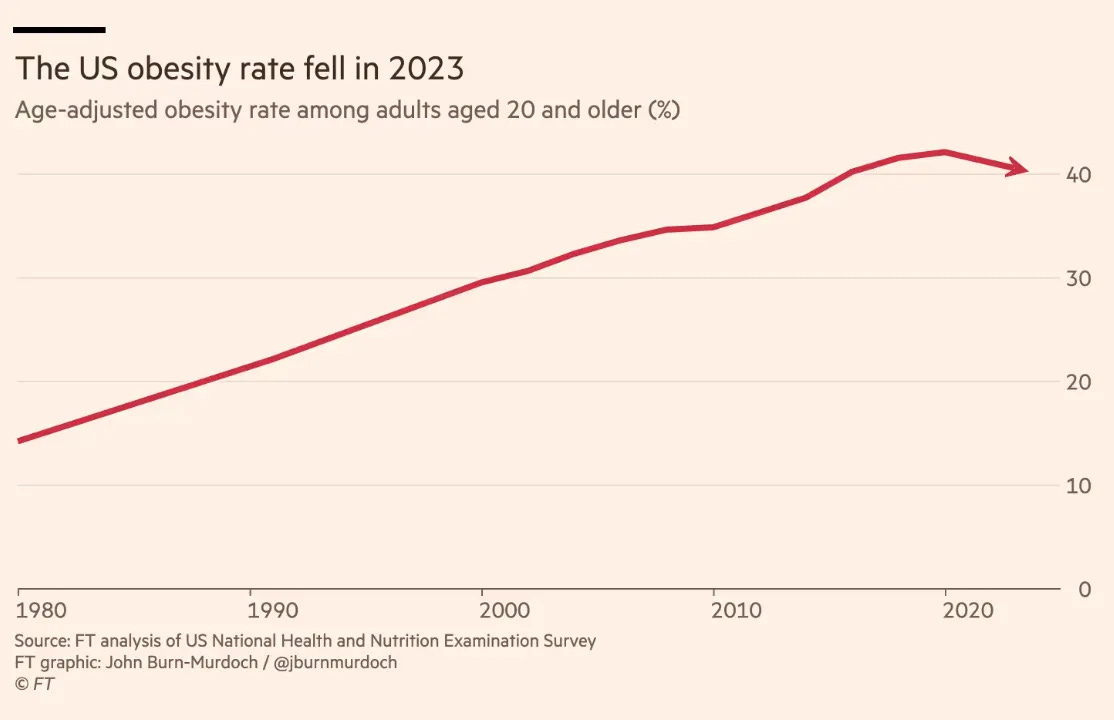
In many ways, the field of addiction today is where obesity was 10 years ago, with low hopes and aspirations for medical progress. In 2014, there were several FDA-approved medications for obesity, but they had low efficacy and were unpopular with patients. There was pervasive pessimism about whether any medication could safely treat obesity and much debate about if it should be considered a disease at all. But when more effective and appealing medications appeared (e.g., Ozempic), sales exploded. For the first time, we may be seeing obesity decline at the population level.
We should urgently advance therapies that can achieve for addiction what GLP-1s are doing for obesity. Human and animal studies indicate that addictive cravings and substance use are medically modifiable. The same revolution in obesity treatment obesity is possible, in principle, for addiction; in fact, similar brain regions that drive cravings for food also appear to drive cravings for other substances.
There are promising addiction drug candidates at many stages of development. Even a modestly increased private-sector investment in addiction innovation might quickly pay dividends to society. If new treatments were to find commercial success, more pharmaceutical companies would enter the space, and successive generations of treatments could help more patients.
The interest in GLP-1RAs for substance use disorders illustrates both the medical potential of the addiction medicine field and its dysfunctional market dynamics. Medications like Ozempic and Mounjaro have shown anti-addictive effects across substances (alcohol, opioids, nicotine, and stimulants) in animal trials, observational studies, and even early-stage human trials. Because of their high efficacy and evident appeal to patients, GLP-1s have potential as an addiction treatment, and are already being prescribed off-label for substance use disorders by physicians and addiction specialists. However, larger Phase 3 trials of GLP-1s for addiction are necessary for strong evidence of efficacy and FDA approval for these indications, which would then unlock insurance coverage and broad patient access. However, because of the industry avoidance of addiction medication research, the companies that hold patents on the medications — Novo Nordisk and Eli Lilly — have not and do not plan to perform Phase 3 trials for this disease. At the same time, government agencies are not structured to step in and advance studies in this situation. The end result is that a promising addiction medicine candidate is stuck in an indefinite limbo.
To fix the market failures in addiction medicine, we propose a series of policy interventions that could accelerate progress towards high impact treatments. If successful, these might ultimately save millions of lives and potentially billions of dollars.
Building a robust market in addiction medicine development
Market Shaping Interventions
1. Expand the FDA priority review voucher (PRV) program to include addiction medicine.
Other disease areas that have suffered from a lack of investment have been successfully incentivized through the FDA priority review voucher (PRV) program, enacted under the Bush administration in 2007. The program rewards companies that get a drug approved in certain categories with a voucher that can be used on different drug applications to accelerate FDA approval (without reducing approval standards), shortening review time from ~10 months to ~6 months. These vouchers are transferable, and currently sell for an average of $100M. The program has spurred the development of drugs for rare pediatric disease, tropical disease, and certain emerging infectious diseases — all areas of medicine that face underinvestment from the pharmaceutical industry.
The vouchers are an important revenue source for companies pursuing neglected diseases and play an important role in decisions to pursue development programs. The PRV program doesn’t require any government spending, but makes drug development in the designated categories more financially appealing. Importantly, vouchers are only provided to drugs that represent a significant advance (as one recent voucher rejection demonstrates), preventing companies from exploiting the program.
We propose expanding the PRV program to cover substance use disorder indications. Doing so would increase the incentive for pharmaceutical companies to develop medications for addiction. Expanding PRV indications has precedent — the program has already been expanded twice, adding rare pediatric diseases in 2012 and Ebola in 2014.
The PRV program has proven successful. For example, it transformed development of medications for rare pediatric diseases (RPD), leading to a surge in approvals of medications for these conditions:
“A total of 53 RPD PRVs have been awarded as of April 30, 2024, reflecting a steady upward trend in rare pediatric disease drug development since the program was first authorized in 2012. Among the 39 rare pediatric diseases for which vouchers to treat those conditions have been awarded, only three of those rare pediatric diseases had any FDA-approved products on the market before the program’s enactment.
“Looking deeper into the drug development pipeline, the trend is even more encouraging. From 2012 to 2022, as many as 569 drug candidates were designated by FDA as rare pediatric disease drugs, with the vast majority designated since 2019. This promises a further increase in RPD PRV awards in coming years.”
With only a tiny percentage of substance use disorder patients willing to take existing medications for alcohol use disorder, cigarette smoking, and opioid use disorder, these indications are effectively orphaned. For cocaine and methamphetamine use disorders, there are zero FDA-approved medications available, despite tens of thousands of overdose deaths per year.
As a neglected market with urgent unmet medical and public health needs, addiction medicine is a good fit for the PRV program. Doing so would likely increase medication development activity, without requiring new government spending.
2. Extend exclusivity for addiction medicines and incentivize pursuit of new indications
When drugs come to market for any indication, they are covered by a combination of FDA market exclusivity rules (12 years for biologics and 5 years for small molecules) and patents (20 years, but the clock starts before the drug goes into trials and can be extended in various ways). The exclusivity period of a medication is the most profitable time for the owner. Finding ways to extend exclusivity is a primary focus of pharmaceutical companies and has large financial implications. Providing additional exclusivity duration increases the ROI on drug development.
We propose extending the duration of exclusivity for alcohol use disorder, opioid use disorder, stimulant use disorder, and smoking cessation, and offering consideration for accelerated approval to medications for these disorders. Specifically:
Addiction medicine indications would receive an additional 2 years of exclusivity for biologics and 3 years for small molecules.
Companies that achieve an indication for a substance use disorder for a medication that represents a significant advance would receive an exclusivity voucher that can be transferred to another medication. For 2nd, 3rd, and 4th SUD indications with the same compound, companies would be granted a shorter duration exclusivity voucher. Durations would be tiered, as described in this proposal from Duke, to balance public interest and reward levels.
FDA should provide increased consideration to addiction medicines for breakthrough, fast track, and priority review designations. FDA should also offer accelerated meeting timelines and responsiveness for addiction medicine developers, which can reduce development costs without compromising approval standards.
Part B above would strongly incentivize companies that have GLP-1s therapies like Ozempic or Mounjaro to repurpose these drugs by pursuing indications for alcohol use disorder, opioid use disorder, stimulant use disorder, and smoking cessation. The benefit to the drug companies of an additional 6-9 months of exclusivity for their GLP-1s for obesity, diabetes, etc. would be substantial. Drug repurposing is a highly efficient strategy, as it builds on the established safety track record of a medication, reducing development costs, shortening time to market, increasing likelihood of approval, and increasing likelihood of long-term safe use in the market.
There are already a number of FDA programs that extend medication exclusivity in specific circumstances, including “orphan drug exclusivity,” which provides added exclusivity for rare diseases, and the qualified infectious disease product (QIDP) program, which provides priority review, fast track designation, and an extra five years of market exclusivity for antibiotic development. Like rare diseases and antibiotics, addiction is a market that requires additional incentives to function effectively.
3. Modernize FDA standards of efficacy for substance use disorder trials
A significant barrier to pharmaceutical innovation in substance use disorders is FDA efficacy standards for substance use disorders that are outdated or unpredictable. Efficacy expectations for substance use disorder indications have been rooted in binary measures, like abstinence, that the scientific and medical community have moved past when evaluating substance use disorder harms.
An article in the American Journal of Drug and Alcohol Abuse argues that binary outcome measures like “number of heavy drinking days” underestimate the efficacy of treatments. And a recent report from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) on alcohol trial endpoints recommends a shift away from abstinence-based endpoints and towards more meaningful consumption-based endpoints. The FDA should adopt this approach for alcohol, and more broadly, for all substance use disorders.
In a recent article in the American Journal of Psychiatry, Dr. Wilson Compton and Dr. Nora Volkow (Director of NIDA) examine the evidence that use-reduction for cannabis and other substances is clinically meaningful and important as an endpoint. They emphasize that the FDA’s insistence on abstinence as an outcome reduces industry activity to develop new medications:
“While achieving continuous abstinence has been documented to be clinically beneficial, such an outcome is difficult to achieve or sustain and is made particularly challenging as the brain circuits involved with self-regulation and stress reactivity have been compromised by drug use. Moreover, the weakening of social and economic support systems that many people with substance use disorders face imposes further barriers to abstinence. Such a difficult-to-achieve outcome has deterred the development of new agents to treat substance use disorders.“
For a recent example, in the Phase 2b trial of a cannabinoid receptor 1 agonist for cannabis user disorder, the FDA required a standard of efficacy of an 80% reduction in use. The trial was unsuccessful by any standard, but several researchers in the field expressed frustration to us that this requirement, a reduction far beyond that required to improve a patient’s health, sends a negative signal to other companies interested in advancing effective addiction treatments.
There are signs the FDA has begun to modernize their approach. A recent joint NIH and FDA paper on smoking cessation therapies provides updated guidance that moves in the right direction.
More broadly, the FDA should work to adopt endpoints and standards of efficacy that align with standards in other disease areas. This shift would be best achieved through new guidance or statements issued by the FDA, which would offer positive assurance to pharmaceutical companies that they have achievable paths to approval. Predictability throughout the medication development life cycle is critical for companies considering investment.
To encourage the FDA’s evolution in this direction, Congress should include statements in upcoming appropriations and authorizations that state:
The FDA should adopt non-binary use-reduction standards of efficacy for addiction treatments that are aligned with standards for other common disorders and the FDA shall, within 12 months, report on the standards employed for substance use disorder relative to other prevalent chronic conditions and report steps to eliminate disparities in evidentiary standards and issue new guidance on the subject.
The FDA should publish clear guidance on endpoint targets across substance use disorders to support decision-making for pharmaceutical companies considering work in this field.
4. Advanced purchasing or risk sharing for candidate medicines
Uncertainty around market size and payer coverage deters private sector investment in addiction medicine. The federal government should offer advanced commitments for particularly promising SUD candidate therapies to address this concern. These commitments could come in the form of formulary inclusion, advanced purchases, or minimum sales guarantees, as appropriate. The proposed PASTEUR Act, which would offer incentives in the form of subscription contracts for development of new antibiotics, could be a model here.
These commitments would only be offered for drugs in development that have a strong likelihood of transformative impact — as with FDA decisions on PRVs, minor changes within existing drug classes would not receive these kinds of guarantees. A group of (financially non conflicted) experts modeled after FDA advisory committees could be charged with developing the guidelines under which these guarantees would be extended.
As an example, suzetrigine is a new non-addictive sodium-channel painkiller that is expected to be approved by the FDA in early 2025. It has efficacy comparable to Vicodin and could replace opioids for pain relief for many situations. However, suzetrigine will arrive with a high on-patent price, and payers will generally deny coverage unless a patient has tried and failed opioids for pain. As a result, doctors will continue prescribing opioids even when they would prefer to prescribe a non-opioid option, and this will lead to new opioid use disorders. Advanced purchasing for opioid-replacing medicines like suzetrigine could provide a mechanism for offering broad access that is affordable for the government, benefits the public, does not overpay relative to value, and does not discourage medication development.
Alternatively, a prize model could provide companies with cash for achieving specified breakthroughs in addiction medicine. Prizes are growing in use as a mechanism for government to incentivize innovation. This might be structured as an annual $500 million pool to reward companies for bringing high-impact anti-addiction and non-addictive pain medications through to market.
Public funding and strategy interventions
5. Increase public funding for addiction medication development
The aforementioned policies are directed at a later stage in the R&D process, and designed to “pull” innovations along into commercialization faster. This has the important advantage of attracting private investment and talent. However, there is also a “push” side to the equation: the basic science of addiction needs more funding to identify good drug targets and bring them into clinical phases. Sustained federal-level investment in addiction medicine research and development will ensure that the field has a strong pipeline going forward.
Currently, the US government allocates less than approximately $700 million annually to addiction medication development — which is too low given the vast medical and social cost of addiction.
Total funding for National Institute on Drug Abuse should be increased from $1.8 billion to $4 billion, and NIAAA’s budget should be increased from $600 million to $1billion. This would bring total funding for addiction research to ~$5 billion, closer to the levels of the National Cancer Institute ($7 billion) and NHLBI ($4 billion), commensurate with the level of harm that addiction inflicts and the value of intervening upstream.
The new funding should be focused specifically on acceleration of medication development, and deployed with an agile approach. For example, in addition to pursuing new approvals, funds should be used to study long-term follow-up and to track addiction therapy efficacy and downstream impacts (incarceration, employment, etc.) over multi-year periods. These impacts are rarely studied for addiction therapies but are an essential metric for public health decision-making. In number of deaths alone, substance use disorder qualifies as a problem with the urgency of heart disease or cancer. Adding in the negative externalities of addiction to others — crime, incarceration, and disrupted communities — raises that urgency further. Better data on the impact of current and future substance use disorder medicines on these downstream metrics is essential.
6. Strategy-first funding orientation
Current and additional federal funding for medication development must be strategically deployed. In general, federal research funding programs are designed to respond to proposals from researchers rather than to be proactive in pursuing a research question or project.
Due to the lack of pharmaceutical activity, funding agencies that focus on addiction medicine should orient towards a more active posture. That means developing and rapidly advancing high-priority research questions and offering large grants with rapid turnaround when needed. As we saw with the $350 million HEALing Communities Study, NIDA has the capacity to drive major investment towards centrally defined strategic priorities. It should do so more frequently.
By developing ongoing mechanisms and funding pools, this can become part of agencies’ workflows, with particular focus on promising medication classes and candidates. This approach will help advance the highest ROI opportunities with the ability to pivot large amounts of funding quickly into areas that show exceptional promise.
7. Public-private partnerships for drug development
The NIH should actively seek public-private partnerships that bring together government funding, academic expertise, and the experience of pharmaceutical companies to help bring treatments to market. Addiction could be added to the NIH Accelerating Medicines Partnership (AMP), which works across nine other disease areas and collaborates with dozens of pharmaceutical companies.
The Cancer Moonshot and Operation Warp Speed are more specific examples of public-private funding and collaboration that have accelerated medication development. This “strategic blueprint” for antibiotic development outlines partnership approaches that can manage risks, share resources, and accelerate the pipeline. Many of these models would also work well for substance use disorder development efforts.
For example, if a pharmaceutical company has a potentially promising treatment in its portfolio but is averse to running trials on patients with opioid use disorder, it could be paired with a federal agency like the Department of Veterans Affairs (VA) that can manage trials while providing some brand independence.
Measuring success and costs
How will we know if we’ve succeeded?
In terms of industry activity, a specific target is a healthy pipeline of multiple phase 3 programs underway at any given time. For the outcome of successful FDA approvals, we can use antidepressants as a benchmark, since the number of Americans with depression is around 18%, similar to the roughly 17% who have a substance use disorder. There are more than 30 in-market antidepressants, but only about seven for substance use disorders. If these policies are successful in reviving the market for addiction medicine, we should hope to eventually match the range of options in the antidepressant market.
Another metric is increasing patient adoption. Substance use disorders and depression have similar prevalence, yet only 3% of people with substance use disorders take medication, 0.5% of the population. Meanwhile, at least 13% of Americans (and likely more) take antidepressants — a 26x higher adoption rate than substance use disorder medications. Until we can increase the appeal and adoption of SUD medications by at least 10x, we won’t be on track to make population-level impacts.
The total cost of a legislative package for what is proposed in this plan is roughly $3 billion annually. Several of the proposals are low or no cost. Compared to the tens of billions we spend each year on the downstream costs of addiction and the trillions in annual economic costs, this plan could end up saving money on net over time.
We can’t solve addiction if we don’t try
Addiction, cancer, and heart disease are the largest drivers of death and disability for Americans (and a large portion of those cancer and heart disease deaths are caused by substance use). Heart disease and cancer have seen substantial breakthroughs in recent years, due to ongoing focus from pharmaceutical companies, paired with a sustained commitment to basic science funding in those areas. Meanwhile, addiction medication has stagnated for decades. Advancing the pace of discovery and development in addiction medicine has the potential to save hundreds of thousands of lives domestically, millions globally, substantially lower disability and disease burdens across societies, and reduce crime and distrust.
There may be no realistic alternative that can reduce addiction at scale: our best prior policy efforts have not delivered the breakthroughs we’ve hoped for and need. Our best path forward is through innovation.
APPENDIX: Innovation is happening in the illicit market but not in treatment development
The core driver of the rapid increase in overdose deaths over the past 15 years has been the dramatic growth in the supply of fentanyl and the rapid decline in cost of methamphetamine. This represents a period of rapid innovation and growth in the illicit drug market at the same time that we have experienced profound stagnation in the development of medications to reduce addictive drive and consumption.

Fentanyl
Fentanyl is a synthetically produced opioid, made from commercially available precursors and much cheaper to produce than heroin. Fentanyl is also much stronger, making it far easier to smuggle: one can hide 8,000 doses of fentanyl inside one golf ball. Reporters at Reuters recently bought $3,600 worth of fentanyl precursors online, enough to manufacture $3 million worth of fentanyl, to demonstrate how easy the process is.
Existing medications for opioid dependence and overdose are less effective for fentanyl than they are for heroin. Research on opioid treatment effectiveness from more than 8 years ago, when fentanyl was relatively rare, may be inaccurate today as fentanyl dominates, because fentanyl is substantially different from heroin:
Fentantyl is so much stronger than heroin that it is easy to combine with other drugs and now over 30% of overdoses are intentional or accidental combinations (see the chart above).
Fentanyl wears off more quickly, so people who use fentanyl redose more times per day than those who use heroin and often combine fentanyl with methamphetamine to extend the time before they need to redose.
Fentanyl is ~25x stronger than heroin, so it is easier to accidentally take too much and overdose.
Naloxone, aka Narcan, reverses opioid overdoses but doesn’t work as well with fentanyl compared to heroin (a better option is becoming available now, but is not yet widely adopted).
In addition to the limitations of existing opioid treatment medications, some long-term rehab strategies that showed promise for heroin addicts may be counter-productive today, since fentanyl kills so quickly. Many people die before ever becoming a long-term user or “hitting rock bottom.”
Canada has long been praised for offering better access to medications like methadone and suboxone and making it easier for people with opioid use disorders to access recovery services. For decades, Canada’s per capita opioid overdose rate was just a fraction of the US rate. However, as fentanyl has grown to dominate the illicit opioid supply, Canada’s overdose rate has rapidly converged towards the American rate. Fentanyl steamrolls existing policy and treatment interventions wherever it appears.
Methamphetamine
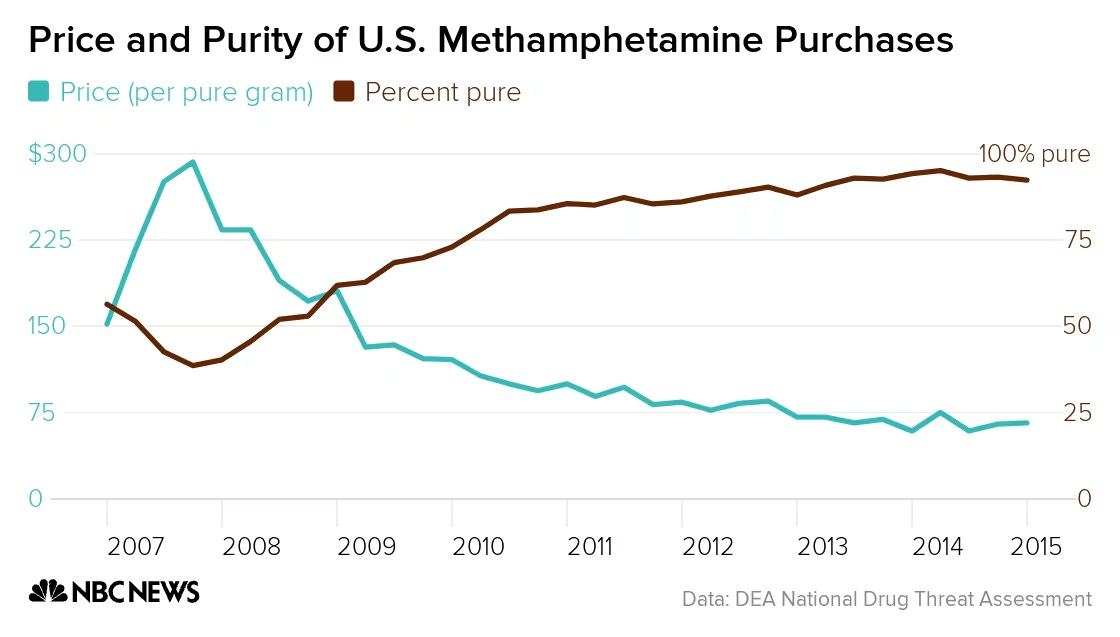
Methamphetamine prices have rapidly fallen as strength has increased, due to breakthroughs in production techniques in Mexican meth labs. The DEA has highlighted the presence of “super labs” in Mexico capable of producing hundreds of pounds of meth per batch.
Meth seizures at the US–Mexico border have seen sharp increases in recent years. According to CBP, meth seizures increased 93% from 2018 to 2019, reflecting the surge in production and smuggling from Mexico. In 2020, CBP seized a record 177,000+ pounds of meth at the Southwest border, up from just 29,000 pounds in 2012. This reflects a more than 500% increase in less than a decade.
The price of methamphetamine in the US has dropped dramatically due to oversupply, with the average price per pound of meth falling from $10,000 to $1,000 in some regions over the past decade.
RAND estimates that street prices for meth fell from $500 per gram to $190 per gram from 2008 to 2016.
The purity of meth has also increased, with DEA data from 2019 showing that the average purity of meth seized was around 97%. This is a direct result of the large-scale, industrial production methods now employed by cartels in Mexico, particularly through the P2P method.
Meth trafficking, which was once concentrated in the western US, has now spread across the country. The Midwest, South, and even New England have seen dramatic increases in meth availability as Mexican traffickers have expanded their networks to new regions.
An increase in use and the combinability of methamphetamine with fentanyl have led to the spike in overdose deaths related to stimulants and opioids, as seen in the purple portion of the overdose chart above.
The combination of larger-scale production, easier access to precursor chemicals, and higher demand has led to a dramatic increase in meth smuggling into the US.

Authors
Executive Director, CASPR
Biotechnology Fellow, Institute for Progress
Adjunct Fellow, Manhattan Institute
Collaborators
Thank you to the following people who reviewed, edited, and contributed significantly in many ways to the development of this publication, and to the many others who contributed off the record.
Will Bainbridge, Premier Consulting
Morris Birnbaum, MD, PhD, University of Pennsylvania
Sona Chandra, President, Pangea Bio
Frank David, MD, PhD, Tufts University and Pharmagellan
Noah Davis, CASPR
Caroline DeBerry, Tenagrity Solutions
Karam Elabd, MSc, CASPR
Alex Jutca, Allegheny County Department of Human Services, CASPR
Lindsay Holden, CASPR
Tom Hudzik, PhD, ALA+ BioPharma Consulting, CASPR Advisory Board
Keith Humphreys, OBE, PhD, Stanford University
Marlene Lira, MpH, Workit Health
Erik Martin, Federation of American Scientists
Sean Riley, Ohio State University
Santi Ruiz, Institute for Progress
Will Schachterle, PhD, Astellas Pharma
Holmes Wilson
Anne Zheng, PharmD
 | A guest post by
|