



GRACE for OUD: Proposing a new GLP-1 based harm reduction strategy
Immediate-access craving relief therapy can bridge the gap between harm reduction and treatment for people at risk of opioid overdose.

Opioid overdoses caused 81,083 deaths in the United States in 2023, nearly double the 2016 rate. Existing policy and treatment programs are failing to achieve significant population level reductions in overdose incidence.
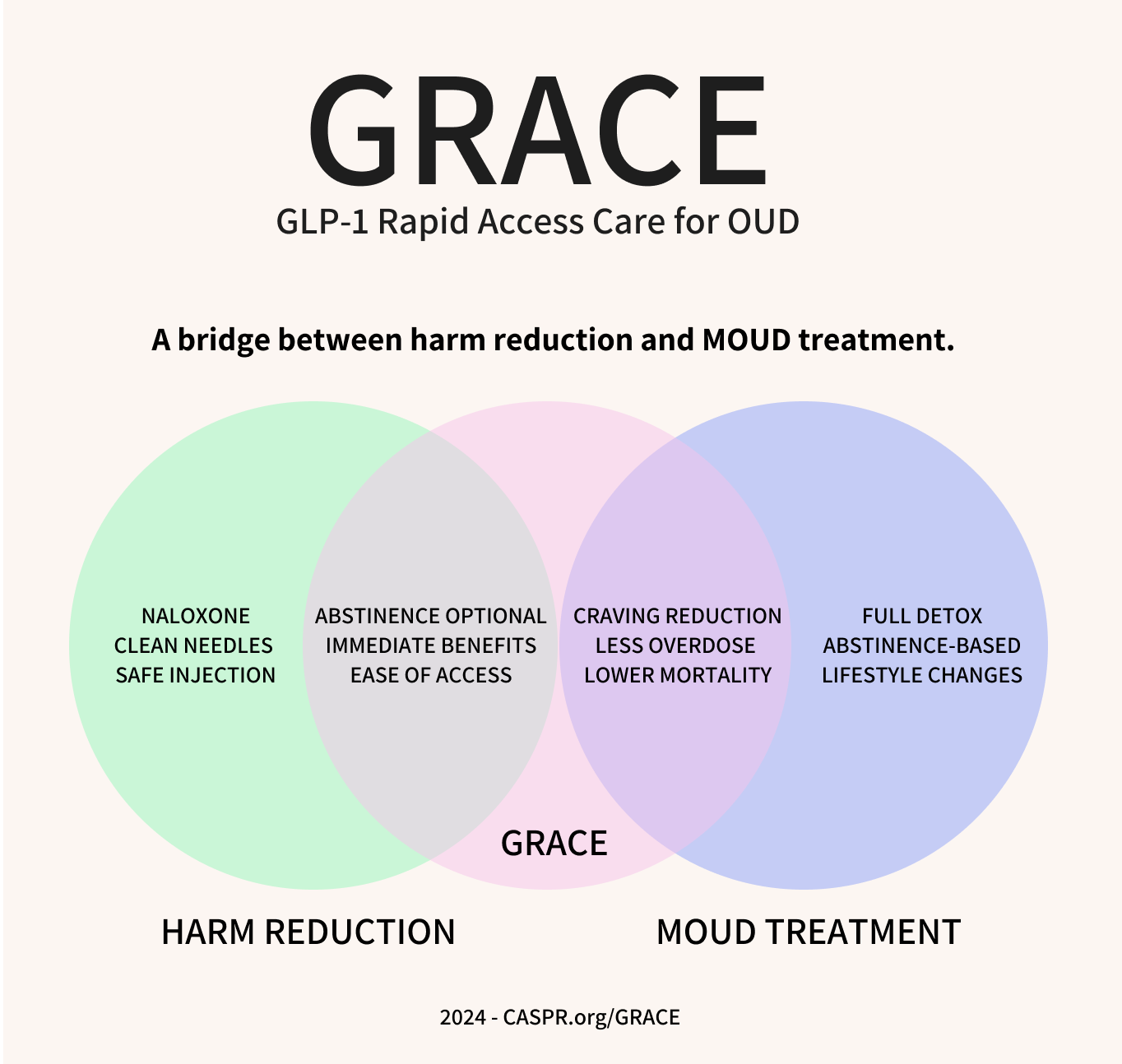
GLP-1 Rapid Access Care (GRACE) for OUD is a proposed model of opioid harm reduction that would provide immediate access to GLP-1RA craving reduction treatment for people with OUD without the obstacles to initiation of opioid agonist therapy (OAT) and without requiring abstinence. GRACE can bridge harm reduction and treatment and can be deployed in settings where medication for opioid use disorder (MOUD) treatment initiation has not traditionally been possible. This model has the potential to reduce acute harms of OUD, improve patient outcomes, and expand the percentage of people with OUD who initiate and sustain treatment. Also see our proposal of GRACE for Alcohol Use Disorder (AUD).
GLP-1RAs reduce opioid cravings and OUD incidence
Cravings are a painful and chronic effect of prolonged opioid use. GLP-1 receptor agonists (GLP-1RAs), such as Ozempic and Mounjaro, have shown significant evidence in reducing opioid cravings and substance use, in randomized controlled trials, real-world patient health record studies, and animal models. The efficacy of these drugs appears likely to exceed that of existing medications for substance use disorders.
For OUD, the GLP-1RA liraglutide has been shown to reduce opioid cravings by 40%, with efficacy seen even at the lowest doses. Newer and stronger GLP-1RAs such as semaglutide and tirzepatide have even greater potential. These medications are already being prescribed by physicians for OUD and AUD, including at leading substance use disorder (SUD) treatment clinics like the Caron Treatment Centers.
More important than just the increase in effect size of GLP-RAs is the potential to dramatically increase the number of people who take and continue to take medications for OUD. Only 13.4% of people in the US with OUD receive medication, because most MOUD options are unappealing to patients and complicated to access. GLP-1RAs offer numerous advantages, including ease of initiation, ease of discontinuation, lack of regulatory restriction, lack of dependency, lack of abuse potential, lack of opioid-agonist therapy (OAT) side effects, mitigation of suicidality, and improvements to mental health.
We strongly encourage you to read our article GLP-1RAs for Addiction: the Medical Evidence for Opioid, Nicotine, and Alcohol Use Disorder, which is the most comprehensive review available of the scientific and strategic advantages of these medications and which provides academic references for the evidence discussed above.
GRACE: GLP-1 Rapid Access Care

The GRACE model, proposed here, would offer immediate point-of-contact dosing of GLP-1RAs for people with OUD or high risk of opioid overdose.
GRACE consists of the following:
Potential recipients would be identified at harm reduction centers, emergency rooms, addiction clinics, or through street outreach programs. GRACE has particular potential for individuals who have been reluctant to initiate treatment in the past or individuals who do not believe they have an OUD, and therefore are unwilling to begin opioid agonist therapy.
Individuals who are presenting with OUD or a recent opioid overdose would be offered GRACE. The harm reduction benefit presented to recipients would be the rapid reduction in opioid cravings that many people experience upon GLP-1RA initiation as well as the long-lasting reduction in overdose likelihood (GLP-1RAs such as semaglutide and tirzepatide are dosed weekly). Potential side effects would be described to patients along with support for initial side effect management (most GLP-1RA side effects subside after the dose escalation period).
Patients who accept GRACE would be given an injection of semaglutide or tirzepatide during their initial encounter. They would also be given the remaining 3 additional injection pens to take home for the rest of the month’s dose. Monthly dosing will continue from there.
Patients would be given information to receive ongoing monthly refills and a phone number for ongoing support by text or voice. Patients would also be provided with ondansetron tablets to take home for nausea management, and potentially additional opioid withdrawal management medication, given the expected reduction in opioid consumption. Providing tablets directly rather than a written prescription will increase ease of use for vulnerable populations. Patients who are identified in emergency settings would follow-up with more traditional providers rather than return to the ER for refills.
For patients who are reachable by phone, providers will conduct follow-up communication via telephone and text messaging to monitor treatment adherence and encourage patients to attend subsequent appointments. Patients would be encouraged to follow up for additional OUD treatment and assessment, but would not be required to make monthly in-person visits to receive GLP-1RA refills unless providers had specific concerns. Ease of use and access is paramount both for individual patient continuation and for building the appeal of the program for potential new participants.
Potential Medical and Strategic Benefits of GRACE
GRACE offers a number of potential benefits to patients, providers, and harm reduction programs:
GRACE has the potential to engage individuals who have the highest likelihood of imminent adverse outcomes. Immediate initiation during an ER visit, at a harm reduction facility, or at a street based mobile clinic reaches people at elevated risk of overdose.
GRACE offers a rapid and appealing benefit by reducing the extreme discomfort of opioid cravings. Craving is a chronic and painful state for people with opioid use disorder and GLP-1RAs offer rapid relief for many people. Providing that relief, along with other harm reduction services, centers the patient and their personal agency while also increasing their short-term safety. Penn State researchers have reported that GLP-1s for OUD appear to have significant craving reduction effects even at the lowest doses. Most patients will see a benefit from the first dose.
Unlike buprenorphine and naltrexone, GLP-1s can be administered immediately, without a detox period. This gives providers a chance to initiate treatment at the point of contact. This may dramatically increase the rate of treatment initiation.
GLP-1RAs do not require abstinence and do not maintain an ongoing opioid dependence. For the vast majority of patients who are hesitant to initiate traditional treatment, removing the requirement of abstinence and providing ease of discontinuation increases likelihood of adoption.
GLP-1RAs can be self-administered at home with no restrictions and no risk of misuse. A patient can be provided a one-month or longer supply of a GLP-1RA at first visit. This makes long-term adherence more achievable.
GRACE provides both immediate relief and ongoing treatment. By reducing cravings, GLP-1RA treatment may also increase the likelihood that patients are able to achieve the detox periods required to initiate on buprenorphine and/or naltrexone, which are compatible with GLP-1RA therapy and are now being studied in combination.
GRACE can operate within a mobile service model for street-connected individuals. Because GLP-1RAs can be administered anywhere, are dosed only once a week, and have no risk of abuse, they could also be provided through weekly pop-up approaches in high risk areas.
GRACE can be incorporated into existing harm reduction programs that have been unable to offer on site MOUD treatment initiation because of detox requirements and/or security risks of stocking methadone and buprenorphine.
GLP-1RAs require only weekly administration, which provides a long-lasting benefit from the initial administration. Long-acting formulations of buprenorphine require clinician administration and cannot be self-dosed. Methadone requires daily visits to clinics which is logistically impossible for many patients.
GLP1-RAs are not opioid-based and do not carry regulatory restrictions or burdensome clinician training requirements.
GRACE provides holistic health and personal benefits to patients by reducing cravings, improving metabolic health, and reducing anxiety, depression, and neuroinflammation.
GRACE has a low staffing and financial burden for providing organizations. GLP-1RAs do not require patients to stay in a facility for any amount of time and therefore demand a far lower burden of initiation management from staff. A very large number of patients could be served by a small team. This can dramatically increase the number of locations where treatment becomes available.
GLP-1RAs can be provided without a high burden of patient tracking or consistency of delivery location. Many OUD patients have unstable housing and transportation and may have difficulty returning regularly to the same treatment facilities. This is an obstacle for adherence to opioid-replacement therapies like buprenorphine and methadone. GLP-1RAs have no potential for abuse and therefore any patient requesting a GLP-1RA can be administered a dose without concern that they are visiting multiple facilities to receive multiple doses. Patients can be welcomed, trusted, and supported, which is beneficial for building a lasting relationship, encouraging adherence, and improving outcomes.
In sum, craving relief through GLP-1RA dosing at the point of contact may vastly increase the appeal and benefit for patients considering initiation of MOUD and may increase the likelihood of continuation of MOUD treatment. GRACE provides a clear short-term benefit to patients, centers their agency, does not require abstinence, and puts them in control of their medication dosing. It may also reduce the cost and staffing burden of treatment provision.
I-GRACE: Incentivized Adherence
Lightweight incentivization of adherence along with GRACE may be able to increase efficacy. Participants would be provided small rewards for visits where they receive GLP-1RA doses.
There is strong evidence showing that contingency management programs, which give rewards like cash or gift cards for abstinence, increase adherence and improve outcomes for patients receiving MOUD. However, for decades, these programs have struggled to scale. Part of the failure to scale is due to resistance from the public and policymakers to ‘rewarding’ people for not using drugs. This resistance has somewhat lessened in recent years but remains a challenge. The larger obstacle to adoption is cost and complexity— contingency management programs require ongoing urine tests, detailed patient tracking, and must be based in facilities able to securely provide opioid-based MOUD. For patients, regular visits for urine testing and medication receipt become a logistical burden, especially for people with financial or legal obstacles to accessible transportation.
If you remove the abstinence requirement, the operation of an incentive program becomes much simpler and cheaper. A patient who begins on I-GRACE would be given a reward each time they return for a weekly dose or, alternatively, a monthly dose + take home doses. This model requires no additional staffing burden and no drug testing. For example, each patient could be given a gift card after their GLP-1RA injection and be told to come back the following week for another. With urine testing and medication security concerns removed, the process can be done easily in mobile clinics that visit specific high risk areas on a weekly basis.
We will be publishing more soon about the adherence incentivization potential of GLP-1s for addiction treatment (make sure to subscribe below to get our upcoming articles and reports, it’s all free).
GRACE can bridge the gap between harm reduction and treatment
Harm reduction and opioid treatment have often lived in adjacent but separate silos. Sometimes the distinction appears to be philosophical– should we be insisting on opioid abstinence or not? – but underlying this is a purely practical constraint. Existing medications for opioid use disorder (MOUD) are opioid-based and require one of two things:
For buprenorphine or naltrexone, an opioid user must be abstinent from opioids before beginning treatment or they may experience sudden and extreme withdrawal symptoms.
For methadone, an opioid user must be prepared to reorient much of their life around daily visits to methadone clinic, which can be logistically daunting or impossible and is often inconsistent with maintaining employment.
These obstacles, combined with the ongoing difficulty of adherence to these medications, side effects, logistical obstacles to access, and the modest effect sizes have dissuaded the overwhelming majority of people with opioid use disorder from initiating MOUD treatment. Harm reduction programs step into this gap and ask: what can we do to reduce harms without demanding abstinence?
Many aspects of harm reduction methodology were born from the realization that requiring abstinence to receive support can be counterproductive to health and safety. Needle exchange is the quintessential example: rather than trying to block access to any drug use materials, providing people with clean syringes reduces the spread of dangerous infections and has been effective for HIV prevention. Harm reduction focuses on strategies that do not demand abstinence: naloxone distribution for overdose intervention, supervised injection sites, pipe exchange to prevent overdose from synthetic opioid residue, and more.
Because of the difficulty initiating and managing MOUD, harm reduction programs typically refer people who are interested in treatment to other facilities and organizations. Imposing additional procedural steps for treatment initiation on individuals in crisis significantly diminishes treatment uptake, even among those with strong motivations to reduce or cease opioid use.
GRACE has the potential to bridge this gap by providing an immediate benefit of craving reduction while also acting as the first step of treatment for patients who are interested in reducing their use. Evidence from studies of both AUD and obesity indicate that GLP-1RAs may, in fact, be most effective for patients at the highest levels of consumption, bringing them back to safer levels.
GRACE in Street Outreach Programs
For the reasons discussed above, GRACE is particularly well suited for deployment in street outreach and street adjacent harm reduction programs. The recent backlash to harm reduction programs is imperiling many of the efforts that have successfully reduced HIV transmission and have widely distributed naloxone for overdose reversal. Most criticism of these programs stems from frustrations that street homelessness and addiction rates have not been reduced by harm reduction efforts.
GRACE offers the potential to dramatically increase the efficacy of harm reduction programs in transitioning people to more stable lives and away from the extreme risks of street homelessness. By providing immediate and week-long reductions in craving and use, harm reduction outreach efforts can win back supporters who have been frustrated by a lack of progress in reducing the most visible elements of the opioid crisis.
Improving the Cascade of Care
For any chance of success in reducing overdose deaths and the burden of opioid addiction in society, we must bring more people into safe use and treatment.
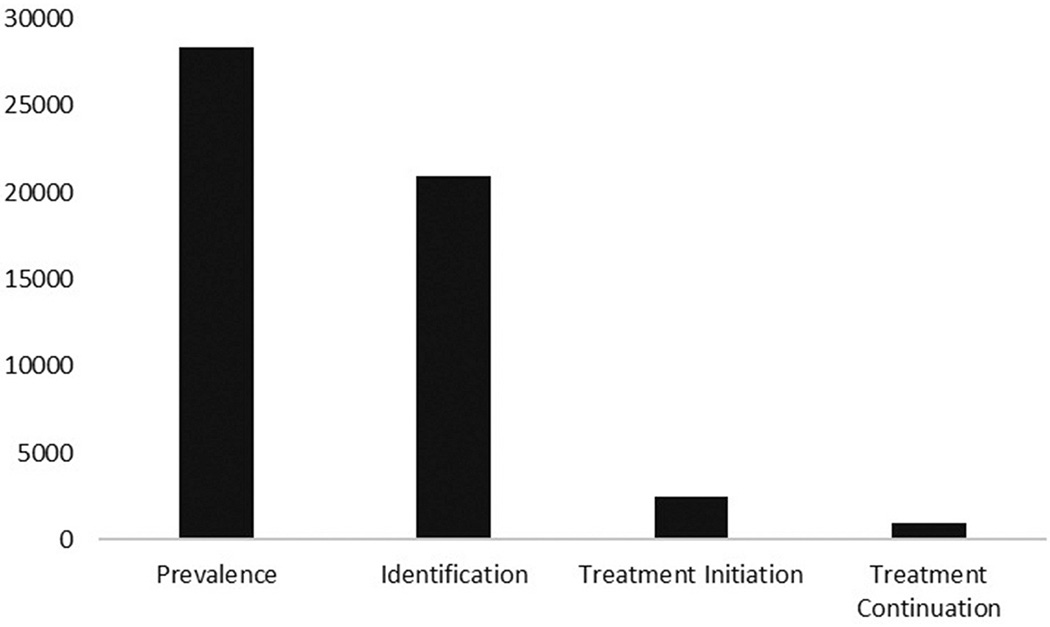
The OUD Cascade of Care model focuses on how many potential patients are actually brought through to treatment. This is what businesses would call their ‘customer funnel’-- how many potential customers actually end up buying the product? For medications for opioid use disorder, the number of people with the condition who end up using medication on a long term basis is very poor.
While national cascade of care data is not available, here is a cascade report of the Florida Medicaid population in 2017 that illustrates the extreme dropoff from prevalence to adherence.
{kind=link}
While Florida in 2017 was not implementing optimal outreach and initiation processes, high drop-off rates like these appear everywhere in the United States and Canada.
Even the US national rate discussed above, 13.4% of OUD patients receiving MOUD in the past year, is only tracking whether patients were dispensed a single dose of medication, not whether patients continued in treatment (the ‘treatment initiation’ step of the bar chart above). The number continuing treatment is far lower. Over 50% of people who begin buprenorphine treatment discontinue within 6 months. Only 13% of private insurance patients still use buprenorphine after 3 years.
Compare this to conditions like diabetes, where 80% of people with the disease (‘prevalence’ in the chart above) are receiving ongoing treatment. GRACE, and GLP-1RA treatment more broadly, can improve performance at each step through the cascade of care.
Potential Challenges of GRACE
Nausea: One common side effect of initiation on a GLP-1RA is nausea and stomach tightness. Nausea is also a side effect of opioid withdrawal and people with OUD are often highly aversive to nausea. Providing take-home anti-nausea medicine such as ondansetron or other withdrawal management medication, as described in GRACE, may reduce symptoms. Ondansetron is already commonly used for both opioid withdrawal symptom management and GLP-1RA initiation. GLP-1RA side effects including nausea typically subside after initial dose escalation.
Weight loss in normal weight individuals: GLP-1RAs have been studied for SUD, Parkinson’s disease, and elsewhere in normal weight individuals. Unwanted weight loss has not been reported as a barrier to treatment so far. Generally, normal weight patients seem to either maintain weight or are able to titrate to an effective dose that doesn’t cause unwanted weight loss. Weight should be tracked in any clinical trials of GRACE to look for potential relevance to adherence or efficacy. Underweight or malnourished individuals should receive additional monitoring, as there could be further weight loss from lack of appetite or, perhaps, weight gain as opioid use decreases and habits normalize.
Cost: GLP-1RAs are covered for diabetes by most payers and for obesity by some payers, with other related indications like sleep apnea coming soon. GLP-1s are currently prescribed off-label for addiction and no payers currently cover this use. Roughly 30% of the US population has obesity or diabetes and can be prescribed with payer coverage on this basis, but that still leaves the majority without coverage. If GRACE is deployed only to people with a covered comorbidity it may still make a significant impact at a public health level. However, achieving broad coverage is essential for reaching the full potential. Long-term, that means phase 3 trials for OUD and AUD to achieve an FDA indication. In the medium term there may be a possibility to receive special discounts / coupons from Eli Lilly, Novo Nordisk, or compounding services, for use in addiction or emergency care settings. Even if patients were given a monthly supply on site and had to return to the site to get more, GRACE would still represent a substantial improvement in ease of access over current treatment options. Also, as additional evidence accumulates, some payers may be willing to pay for GLP-1RAs through GRACE off-label if it is able to substantially reduce the rates of in-patient treatment of addiction. Virtually any intervention that reduces in-patient treatment is cost-saving. From a societal standpoint, addictions have tremendous downstream costs for health care, public safety, violent crime, disability, and death. Even a high cost medication provides a huge financial benefit to the public if it meaningfully reduces incidence.
Diversion: GLP-1RAs are currently experiencing supply shortages. These shortages are expected to ease over the next 9-18 months, but in the near term there could be a financial incentive for some GRACE recipients to attempt to sell take home doses. While brand name semaglutide and tirzepatide have a high sticker price, they are covered by insurance for most current patients and are available from compounded sources for far lower prices. And if GLP-1RA doses are diverted to other OUD patients, this would provide some public health benefit. If this does become a problem, GRACE programs could switch to weekly in person dosing until shortages are relieved.
Next Steps for GRACE
For GRACE to become widely adopted it will require clinical trials and payer coverage. In the short-term, many patients have indicated comorbidities that are already covered by payers. These people could, therefore, receive GRACE affordably today.
Short-Term: Prescribing for Comorbidities
Over 30% of Americans have obesity or diabetes and another 40% are overweight. For these patients, GLP-1RAs reduce mortality and provide additional health benefits. Because GLP-1RAs are already approved for multiple indications, GRACE could be adopted now in clinics or hospitals for patients with indicated comorbidities. Doing so would require the ability to screen patients at the point of contact for GLP-1RA eligibility for diabetes or obesity. This should only be a modest additional burden on ER or clinical staff since GLP-1s are so widely and safely prescribed by physicians in all settings and typically without requiring blood work.
Because of their massive popularity, GLP-1RAs already have a history of safe use in nearly all substance use disorder populations. For example, more people with alcohol use disorder (AUD) already take a GLP-1RA incidentally than take a medication indicated for AUD.
Medium-Term: Clinical Trials of GRACE
To reach broad adoption, GRACE requires clinical trials. A clinical trial of GRACE at an addiction clinic or ER could provide initial real-world evidence. The effect size of GLP-1RAs for addiction has been large enough that even a relatively small trial is likely to show significance. Our organization, CASPR, is interested in partnering with clinics and investigators to run trials of GRACE and we will be approaching NIDA CTN nodes, among others. Please be in touch if you are interested in collaborating.
Long-Term: Phase 3 Trial of GLP-1RAs for OUD and AUD
For full coverage from private and public insurance, GLP-1RAs like semaglutide or tirzepatide require Phase 3 trials and an FDA indication. Funding and running these trials may be the highest ROI opportunity in public health today. Unfortunately, pharma companies have refused to run Phase 3 trials of GLP-1RAs for addiction because of risk aversion and disinterest in the addiction medication market. It may be left to the public sector to advance these efforts.
CASPR, our organization, is part of a developing coalition that is working to bring together a Phase 3 trial of semaglutide or tirzepatide for OUD. Feel free to be in touch if you would like to join this effort. We will be writing more about this soon.
GRACE for Alcohol Use Disorder
While this article is focused on GRACE for people who use opioids, GRACE is equally applicable for people with alcohol use disorder (AUD). Only 2% of people with AUD receive medication, far lower than even the low MOUD usage rates. Offering GRACE for patients in the ER who are intoxicated would reach the population at highest risk of chronic or acute self-harm from alcohol use. GLP-1RAs have demonstrated large reductions in alcohol craving and consumption.
We are eager for thoughts and feedback on GRACE from more providers, clinicians, and researchers. Please be in touch: hello@caspr.org
